|
The cause of bedwetting in children is unclear.
We all wet the bed at age 2 or 3 years, but somehow by the time we are 4 or 5
our brain usually learns to not do so. Children who continue to wet the bed
after that age are believed to either have small bladders, or make more
urine during the night than their bladders can hold, and be overly deep sleepers. Some bedwetters have
an overactive bladder or they have a weak bladder "sphincter", the muscle that controls urine
release. These children usually also wet some during the
day. Ninety-four percent of children with daytime wetting also
"out-grow" it 1.
It makes sense that if a child's bladder overfills, and
he or she doesn't wake up, then a wet bed will result. But studies have shown that children
with bedwetting sleep no more deeply than
non-wetters. There was also another very interesting study in which a group of
children who were not bedwetters were given large amounts of fluid just prior
to going to bed. Six out ten of these children wet that night for the
first time.
So, it appears that most children are just normally deep sleepers, but if they happen to have a small bladder, or make more urine during the night than their bladder can
hold, or they have an unstable bladder or a weak sphincter, then they will wet the bed. That is, unless they can wake up and go to the toilet. Caffeine
tends to make the problem worse, which doesn't appear to make sense, as one would think
that caffeine would make the child sleep less deeply and not wet. But caffeine also causes the kidneys to make more urine, and make it quickly. Children sleep more deeply in the first part of the night, so
that if the bladder fills quickly, there is more chance of wetting rather than waking up.
|
Some
children make
too much urine
during sleep. |
Why do some children make too much urine during sleep? Research has shown that these children
appear to be deficient, during sleep, in a hormone called "anti-diuretic hormone" (ADH).
This hormone normally causes the kidneys to produce much less urine at night than during the day.
Mother
Nature may have designed children to sleep more soundly than adults, so that they don't go wandering around in the dark when their parents are asleep and get hurt.
This works great unless the bladder happens to get overfull. Therefore, it may be that
Mother Nature designed ADH to make children's kidneys produce less urine at night, so they can sleep
all the way through the night without the bladder overflowing. Deficiency of ADH
would then result in too much urine at night for their bladders to hold and a
wet bed. But if
deficiency of anti-diuretic hormone is a cause of bedwetting, then it would seem logical that when a child's bedwetting is cured, such as by a moisture alarm, then the anti-diuretic hormone levels should
have returned to normal. Research has, however, not been able to show this.
| Diapers
may prolong or actually be a cause of both nighttime wetting and daytime wetting. |
 Use
of diapers for bedwetting protection is one way to avoid having to deal with wet sheets, plastic
mattress covers, etc. But at
the recent annual meeting of the American Academy of Pediatrics, Nov. 4, 2003,
approximately 300 pediatricians and nurses in a seminar on bedwetting were asked
how they felt about diapers as a way to deal with bedwetting. Only 15% of the pediatricians and nurses recommended diapers
to their patients for management of bedwetting. Eighty-five percent (85%) of
the pediatricians and nurses, as well as the seminar chairman, Allison
Schonwald, MD of Harvard Medical School, felt that diapers
were not a good idea for kids with bedwetting because diapers, "give the wrong message", namely
that it is okay to wet at night and not get up and use the toilet. It was
felt by most of the pediatricians and nurses, as well as the seminar chairman, that use of diapers, "may prolong
wetting." Use
of diapers for bedwetting protection is one way to avoid having to deal with wet sheets, plastic
mattress covers, etc. But at
the recent annual meeting of the American Academy of Pediatrics, Nov. 4, 2003,
approximately 300 pediatricians and nurses in a seminar on bedwetting were asked
how they felt about diapers as a way to deal with bedwetting. Only 15% of the pediatricians and nurses recommended diapers
to their patients for management of bedwetting. Eighty-five percent (85%) of
the pediatricians and nurses, as well as the seminar chairman, Allison
Schonwald, MD of Harvard Medical School, felt that diapers
were not a good idea for kids with bedwetting because diapers, "give the wrong message", namely
that it is okay to wet at night and not get up and use the toilet. It was
felt by most of the pediatricians and nurses, as well as the seminar chairman, that use of diapers, "may prolong
wetting."
 A
parent on our site suggested an ingenious product called "peej's".
This is a heavy duty pajama bottom with a waterproof exterior. It lets the child feel the wetness without soaking the bed.
The child thus has incentive to hold the urine through the night or get up and
use the toilet. This is not a pant or a diaper. The parent says,
"Somewhat expensive but worth every penny." You can read more
and purchase peej's at the company's website. A
parent on our site suggested an ingenious product called "peej's".
This is a heavy duty pajama bottom with a waterproof exterior. It lets the child feel the wetness without soaking the bed.
The child thus has incentive to hold the urine through the night or get up and
use the toilet. This is not a pant or a diaper. The parent says,
"Somewhat expensive but worth every penny." You can read more
and purchase peej's at the company's website.
Use of diapers may have also other risks. Evidence is
now appearing that emotional attraction to diapers
and diaper "fetish" are quite common in children and teens and may actually be causes of new, recurrent, and prolonged
nighttime wetting and daytime wetting. Also, infertility and even
testicular cancer may be a result of diaper use. (See "Diapers: Are they a good idea?"
below.)
|
How
does mother
nature cure
bedwetting? |
To figure out how to cure bedwetting we really need to understand how a child "naturally" stops wetting the bed.
Treatments that cure bedwetting most likely just speed up what Mother
Nature does to cure them.
Remember, 15% of children who wet will stop on their own each year. This probably happens the same way that a child learns to not wet during the day (in his/her diapers or underwear). It is fairly easy to understand how we learn to hold our urine when we are awake. If we wet in our diapers, it makes them cold and wet, and we also want to not have to use diapers so that we will not be teased by our friends. We thus learn how to stop and start our urine, and we learn to go in the toilet.
But it is hard to understand how we learn to hold our urine when we are asleep, because then we are unconscious. Yet even when we are awake the holding of urine is somewhat unconscious. We are able to concentrate on the last part of a long movie, even though we may have to urinate pretty bad! And when we are asleep we are still partly conscious, because
we turn over, we adjust our pillow, we keep away from the edge of the bed, and
we dream. As a matter of fact,
many kids with bedwetting report that they at times dream that they are in the bathroom, and then they wet.
|
How
does a child
learn to not
fall out of
bed? |
Learning to stop wetting the bed is similar to learning to not fall out of bed at night or
to not throw off the covers. How did  you learn to not fall out of bed? The answer is that after you fell
on the floor a few of times, you
associated the edge of the bed with falling, and thereafter you kept away from the edge of the bed, even though you might be
deeply asleep. But you had to wake up each time you hit the the floor in order to connect the edge of the bed with falling. you learn to not fall out of bed? The answer is that after you fell
on the floor a few of times, you
associated the edge of the bed with falling, and thereafter you kept away from the edge of the bed, even though you might be
deeply asleep. But you had to wake up each time you hit the the floor in order to connect the edge of the bed with falling.
If a child fell on the floor every time he or she wet the bed, most kids would
stop wetting pretty quickly. Mother Nature probably cures kids of bedwetting
with a similar unpleasant experience. When the child is suddenly awakened by urine running down
their leg, followed by a cold, wet feeling, this unpleasant experience is associated with releasing the urine, so eventually it keeps
them from letting their urine go, even when they are asleep, or they may learn to wake up. So, we can learn even when we are at least partially asleep.
Deep sleepers, of course, have a harder time learning this. But even deep sleepers can learn to hold their urine or wake themselves and go to the toilet.
In war, for example, exhausted soldiers, dead asleep in the trenches, can learn to awaken at the first sign of an attacker.
This probably happens because of focused concentration.
|
The
key seems to
involve waking
just as the
urine is let
go. |
Again, the key to learning how not to wet the bed seems to be being awakened just as the urine is let
go by a somewhat unpleasant experience. It appears that we can't learn if we are
totally asleep. The child has to associate releasing the urine with the unpleasant event.
Remember, you wouldn't have learned to not fall out of the bed if you weren't awakened by the fall. The same is true for bedwetting: the child must wake up.
Even though normal children are deep sleepers, most can be awakened by urine running down their
leg and the cold, wet feeling that follows. The child thus learns to hold the urine throughout the night
in order to avoid the cold, wet feeling, or the child learns to wake up and
go to the toilet.
But if a child is
such a deep sleeper
that the wet sheets
don't wake him or her
up, then a moisture
alarm can help.
|
A
moisture alarm
can help the
child wake up |
A moisture alarm is simply a little beeper, worn by the child, that goes off when urine contacts a wired pad in either the child's underwear
or on the sheet underneath. If the child is a moderately deep sleeper then a "moisture alarm"
will often awaken him and help make the association between the urine being released and the
wet bed. Also, because the moisture alarm rudely  awakens the child, it causes
the child to associate releasing the urine with a further unpleasant event
(being jolted awake), in addition to the cold, wet bed. Approximately two thirds of children with bedwetting can be cured with a moisture alarm, within 3 to 6 months.
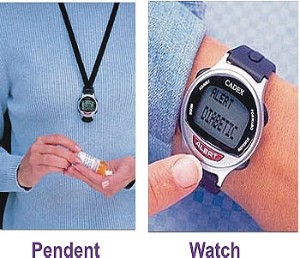
Children who do not awaken to noise alarms will often
awaken to a vibration alarm, such as the Potty Pager or the Palco Wiggler.
Some wetness alarms come with both sound and vibration, such as the Palco Wet
Stop and the Malem alarms. Information on wetness alarms can be found on the Alarms
Page. awakens the child, it causes
the child to associate releasing the urine with a further unpleasant event
(being jolted awake), in addition to the cold, wet bed. Approximately two thirds of children with bedwetting can be cured with a moisture alarm, within 3 to 6 months.
Children who do not awaken to noise alarms will often
awaken to a vibration alarm, such as the Potty Pager or the Palco Wiggler.
Some wetness alarms come with both sound and vibration, such as the Palco Wet
Stop and the Malem alarms. Information on wetness alarms can be found on the Alarms
Page.
If the parent mildly scolds the child when the alarm goes off (because
they have started to wet), this
appears to reinforce the unpleasant association of being awakened when the urine
is released. Similarly, the parent should praise the child when he or she is
able to sleep through the night without the alarm going off, or get up and use the toilet.
|
The
parent must
back the child
up in
awakening. |
If the child sleeps through the alarm, then a parent must backup the alarm. The parent, however, must
wake the child as soon as the alarm starts, which is difficult, so that the child associates the urine release with the alarm and the wet bed.
Rewards and praise for awakening within a certain time such as 15
seconds, also help. Vibration alarms have the advantage that they
frequently wake deep sleepers when noise alarms fail, and they do not disturb the sleep of other household
members. But because they are not heard, they are difficult for a parent to back up.
| "Wake
up training" - Training a child to awaken at night to use the toilet. |
 The most straightforward approach to bedwetting is teaching the child to awaken at night.
If
a child could wake up when his/her bladder is full and then go to the toilet,
this would obviously prevent wetting. Theoretically, awakening is the quickest way to obtain a cure, because it can compensate for a large urine production or a small bladder size.
The smaller the child's bladder, the more important it is for him to learn to awaken at night.
Most bedwetters go to bed thinking
that they have to hold their urine for the
entire night. They do not realize that it is perfectly normal to get up
and use the toilet in the night. Statistically, about 30% of the general population must do so
for their entire life. The child must therefore tell themselves to
“wake up every night and use the toilet." If a child fails
to self-awaken when the bladder is full, and it can be determined what time of
night the child typically wets, a standard alarm clock can be used to awaken the
child just prior to that time. If the child sleeps through a The most straightforward approach to bedwetting is teaching the child to awaken at night.
If
a child could wake up when his/her bladder is full and then go to the toilet,
this would obviously prevent wetting. Theoretically, awakening is the quickest way to obtain a cure, because it can compensate for a large urine production or a small bladder size.
The smaller the child's bladder, the more important it is for him to learn to awaken at night.
Most bedwetters go to bed thinking
that they have to hold their urine for the
entire night. They do not realize that it is perfectly normal to get up
and use the toilet in the night. Statistically, about 30% of the general population must do so
for their entire life. The child must therefore tell themselves to
“wake up every night and use the toilet." If a child fails
to self-awaken when the bladder is full, and it can be determined what time of
night the child typically wets, a standard alarm clock can be used to awaken the
child just prior to that time. If the child sleeps through a standard
alarm, there are very loud alarm clocks (see Sonic
Boom clock at left), which even has a silent "bed-shaker"
attachment (shown at right), which can be placed under the pillow or mattress,
and which will awaken the soundest sleepers, and without
awakening the rest of the house. Learning to pull oneself out of a deep
sleep takes work, and rewards may help. Parental backup sometimes is
required for a short time. Use of a diaper may impair the child's learning
to wake up and use the toilet at night, as there is little incentive to wake up
if the child can simply wet in the diaper. And diapers may have other
risks (See "Diapers: Are they a good idea?"
below).
standard
alarm, there are very loud alarm clocks (see Sonic
Boom clock at left), which even has a silent "bed-shaker"
attachment (shown at right), which can be placed under the pillow or mattress,
and which will awaken the soundest sleepers, and without
awakening the rest of the house. Learning to pull oneself out of a deep
sleep takes work, and rewards may help. Parental backup sometimes is
required for a short time. Use of a diaper may impair the child's learning
to wake up and use the toilet at night, as there is little incentive to wake up
if the child can simply wet in the diaper. And diapers may have other
risks (See "Diapers: Are they a good idea?"
below).
One technique for self-awakening is to ask children to rehearse a particular sequence of events every night before going to sleep.
The child lies in bed with his eyes closed and pretends that it's the middle of the night and his full bladder is trying to wake him up by starting to hurt, or the alarm has gone off.
He then runs to the bathroom and empties his bladder. At the end of the rehearsal, the child can remind himself to get up in the same manner if he needs to urinate during the night.
Many children are surprised to learn that their bladder sends the same signal when it becomes full at night as it does during the day.
"Dry Bed Training" is a more labor intensive technique used to teach children to awaken at night. For this method to be successful, the parent must be committed and consistently available. Here is the standard technique (author unknown).
A weekend or vacation is usually the best time to try this technique, so as not to interfere with sleep needed for
school. 1) On the first night wake the child once an hour until 1 a.m., using the minimal prompt necessary. Try a hierarchy of prompts, ranging from turning on the light to saying the child's name to touching him.
Make sure he is awake enough to walk and talk coherently. If he's dry, praise him and ask. "Do you need to go to the toilet or can you wait another hour?"
He must walk to the toilet on his own. If he's wet, encourage him to change his pajamas and bedding.
At the 1 a.m. awakening, tell the child to void even if he's dry. 2) For the next five nights. wake the child only once. The first night. wake him three hours after he falls asleep.
The next night. wake him two and a half hours after he falls asleep. Keep diminishing the interval, so that on the fifth night you wake him an hour after he falls asleep.
3) On the sixth night, tell him to wake himself from then on. 4) If the child relapses - has three consecutive wet nights - repeat the six nights of awakening.
In a study of 51 children using this technique, the cure rate was 92%. The average length of time to achieve a cure, defined as 14 consecutive dry nights. was four weeks. The relapse rate was 20%, but all the children who relapsed responded to a second course of training.
|
When
away from home
children with
bedwetting wet
less. |
When bedwetters sleep away from home, such as at their grandparents' or at a friend's house, they frequently will not
wet. But once back home they wet again. When away from home, somehow, they either sleep less deeply or concentrate more on not wetting.
The treatment program of one organization, Pacific International Ltd.,
actually has the child temporarily sleep on a piece of plywood under the sheet, which might seem harsh at
first. But they believe it helps the child to sleep less soundly, so that he/she
may learn to awaken to the sound of an alarm or to the feeling of a full
bladder, so they can get up and use the toilet. Or they can learn to hold his/her
urine for the entire night.
|
Why kids have wet or dry nights is not known. |
Even children with very frequent bedwetting usually have some dry nights,
indicating that most do have the ability to be dry. Thus, something about
either their sleep "thoughts" or their urine production changes when
they are dry. It is important to try to identify what is different about the
day before a dry night. Were they less tired? Did they drink less in
the evening? Was the day less hectic? But many kids have a dry or wet night even when they appear to do exactly the same things the day before.
An article in the June 2000 issue of Clinical Pediatrics suggests that the difference between a wet or a dry night
may have something to do with how much salt a child eats. Salt makes the body hold onto water, so that the water may not be
put out by the kidneys for many hours, perhaps not until the middle of the night or even until the next day or night. Keeping a salt intake diary may help to
show the relation to a dry or wet night. Salty foods like chips and pretzles must be counted, as well as table salt.
|
Hypnosis
can cure
enuresis in
some cases. |
Hypnosis is
successful in curing
enuresis in
approximately 50% of
children who try it. This is hypnosis without the "hocus pocus" of
trances. It consists simply
of having the child make mental images of holding his urine when asleep, or waking when his bladder is full, with a lot of positive reinforcement.
|
Bladder
volume
alarming is a
new treatment
method. |
There is a new treatment for bedwetting being investigated called Bladder Volume Alarming. This method uses ultrasound to automatically measure the volume of urine in the child's bladder every few
minutes during sleep. Children generally wet when  their bladder fills to about the same volume. Alarming when the bladder
has just about reached that volume will wake the child and allow going to the toilet before wetting.
Thus, the child stays dry. Also, because the alarm occurs when the bladder is full, the child associates the fullness feeling with the alarm. The child gradually learns to wake up without the alarm when his bladder is full. The advantage of the bladder volume alarm method for treatment of
bedwetting is that the child stays mostly dry during the treatment period. But the equipment for this method is
fairly expensive, and the time required is generally longer than that for other
methods. Bladder Volume Alarming is still experimental. their bladder fills to about the same volume. Alarming when the bladder
has just about reached that volume will wake the child and allow going to the toilet before wetting.
Thus, the child stays dry. Also, because the alarm occurs when the bladder is full, the child associates the fullness feeling with the alarm. The child gradually learns to wake up without the alarm when his bladder is full. The advantage of the bladder volume alarm method for treatment of
bedwetting is that the child stays mostly dry during the treatment period. But the equipment for this method is
fairly expensive, and the time required is generally longer than that for other
methods. Bladder Volume Alarming is still experimental.
|
Medications
can prevent
bedwetting,
although they
do not cure it. |
Antidepressants: Over the years, many different drugs have been used to treat children for bed-wetting, including drugs that are usually used to treat depression (ANTIDEPRESSANTS). While these drugs have helped some children, most have not proven to be an effective long-term cure. The drug in this class that is used most frequently is called imipramine. It has been successful in helping bed-wetting in approximately 30% of children. Antidepressants are powerful drugs and some can have serious side effects, especially in children. They must be used with care, under the close supervision of your doctor.
Desmopressin acetate (DDAVP): DDAVP is a man-made form of antidiuretic hormone that works by substituting for the natural hormone. It helps the child's body make less urine, and thus lessens the risk that the child's bladder will overfill during sleep. DDAVP
is given to the child as a nasal spray or by oral tablets.
Approximately 60% of
children improve
significantly on DDAVP,
although they may
still wet
some. DDAVP is most helpful in children who make too much urine at
night or who have small bladders, and who are also very deep sleepers. It
does not work well in children with overactive bladders 2.
Children with overactive bladders usually also wet some during the day.
Children with overactive bladders are usually helped more by medications that
decrease bladder spasms, such as Oxybutynin (see below).
Few side effects have been reported in children using DDAVP. The main side effect noted has been headache (4%). DDAVP does, however, take control of the child's water balance, so the manufacturer includes a caution statement: "Nighttime fluids should be restricted to decrease the chance of fluid
overload." If a child takes DDAVP and then drinks a large amount of fluids, this
can dilute the level of salts in their blood, and seizures have resulted. Children with certain conditions may require special care in using DDAVP. Your doctor will advise you if your child is in this category.
DDAVP can work quickly. Some children will be dry after the first night of using DDAVP. Many doctors recommend using the medication for 3 months, followed by a tapering off period to determine if the child can stay dry without the drug. The majority of children responding to DDAVP will resume bed-wetting when the drug is withdrawn. If the child becomes wet again your doctor may ask you to restart DDAVP
and try to stop it again every few weeks to see whether your child still needs it to stay dry. Many children use the medication only for overnights or summer camp.
Treating your child with DDAVP is more expensive than using moisture alarms. Costs may range between
$ 60 and $240 per month, depending on the dosage the doctor prescribes. In some cases this is covered by insurance. 60 and $240 per month, depending on the dosage the doctor prescribes. In some cases this is covered by insurance.
Oxybutynin (Ditropan): children with small bladders and children
with overactive bladders may benefit from oxybutynin, which decreases bladder
spasms 2.
These children usually also have daytime as well as nighttime wetting. Oxybutynin
does have minor side effects, the most common of which is dry mouth.
Daytime wetting can also be helped by having the child use the toilet every two
hours. Silent alarm wrist watches
(see right) can help remind the child. (Child
watches $$).
|
The
affect of bedwetting on a
child's
self-esteem
can be
considerable. |
 The impact on a child's social life and self-esteem can be profound. Children with bedwetting are not able to attend sleep-overs or go to camp.
They avoid taking
friends to their
rooms, because of
the smell of urine
there. Many say that they feel "different" from other children, and they fear that they will be humiliated if their
"secret"
gets out. Moreover, in some children, even if they are eventually cured, lasting psychological problems can
result The impact on a child's social life and self-esteem can be profound. Children with bedwetting are not able to attend sleep-overs or go to camp.
They avoid taking
friends to their
rooms, because of
the smell of urine
there. Many say that they feel "different" from other children, and they fear that they will be humiliated if their
"secret"
gets out. Moreover, in some children, even if they are eventually cured, lasting psychological problems can
result
3. The impact on the child's family can also be significant. Divorce rates are higher in families with a bedwettting child. Therefore, because of the social and self-esteem impact, recommendations are now appearing in the medical journals that treatment for bedwetting be started as soon as it
really bothers either the child or the parents.
| Constipation
can cause bedwetting. |
About half of the children evaluated for bedwetting in the Seattle Children's
Hospital Enuresis Clinic are found to be constipated. After relief of
their constipation many of these kids improve or stop wetting. Many of
these children also soil their underwear, and the soiling usually stops after
treatment of the constipation. Why does
constipation cause bedwetting? It is simply a matter of
"space". If the lower abdomen is packed full of stool, there is little space left for the bladder to fill. The restricted
bladder can not hold the normal amount of urine and overflows quickly,
particularly at night during sleep. Also, the large mass of stool pressing
against the bladder decreases the sensation of having to urinate.
What are the signs of constipation? Children who are constipated have
infrequent, large hard bowl movements. Kids should have a bowel movement at
least every two days. Also, children who stay on the toilet for prolonged
periods when they have a bowel movement are frequently constipated. Constipation can even result in chronic
diarrhea and soiling, since the large mass of packed
stool allows only liquid bowel movements to pass around it.
What can be done to relieve constipation? If constipation is suspected,
the child should be seen by your doctor. Significant constipation usually
requires enemas to break up the packed
stool. Treatment is then typically done with stool softeners like mineral
oil (2 tbsp. each morning in yogurt) and
suppositories (Dulcolax) to insure that the child has a bowel movement at least every two
days. If the lower intestine has become over-distended, usually a few
months are required for the intestine to regain its normal function, and recurrence
of constipation is common.
Constipation can be prevented by fruit juices, such as pear juice, and by
fiber foods such as popcorn and shredded wheat (Frosted Mini-Wheats have both
fiber and sorbitol, a non-absorbed sugar that serves as a stool softener).
Restriction of fluids can also be a cause of constipation. Thus it is
important to not restrict fluids to prevent bedwetting if your child shows any
of the signs of constipation. Your doctor can suggest other prevention methods.
| Diapers: Are they a good
idea? |
Putting a child back in diapers may seem like the easiest way to manage
bedwetting. But diapers have some risks...
The October 2000 issue of Archives of Disease in Childhood
raises an alarming concern about the use of diapers in kids. Could the decline in male fertility over the last
twenty or thirty years and the increase in testicular cancer both be due to
the widespread use of plastic-lined diapers that keep the scrotum and testicles of boys too
warm? Mother nature placed the testicles outside of the body,
so that the testicular temperature is normally several degrees cooler than core body
temperature. Disposable, plastic-lined diapers restrict ventilation to the
testicles. The ADC study found that plastic-lined diapers can raise the temperature of the testicles to the level of core
body temperature. The higher temperature may cause abnormal testicular
development and may result in infertility or ever cancer in the future, similar
to what happens in undescended testicles. Cloth diapers (without plastic pants)
were found to keep the testicles at near normal temperature. Cloth diapers with plastic pants were not investigated in
this study, but may also raise the testicular temperature to potentially
hazardous levels. (For additional articles on testicular temperature
hazards of diapers click
here.)
The monthly polls on this site
reveal that more than half of the kids coming to this site want to wear diapers,
but what is startling is that they want to wear diapers FOREVER. More than
50% indicate that diapers are a "comfort" to them, and they do not
want to ever stop wearing diapers. More than 60% indicate that they would
rather wet in a diaper and sleep than wake up and use the toilet in the
night. More than 60% (of 350+ kids voting) indicate that they have wet on purpose so that they would be allowed to wear diapers.
Children do need a fair amount of sleep, but about 30% of "normal"
people must get up and use the toilet every night, for their entire lives.
And statistically, 50% of bedwetters who become dry (e.g. by alarms) do so by
learning to get up in the night and use the toilet. The other 50% learn to
hold their urine for the whole night. But if a child is allowed to wet in
a diaper and  sleep, then there is little incentive to learn to wake up and use
the toilet. There is also little incentive to learn to hold the urine for the
entire night. Diapers may thus prolong nighttime wetting. (See article
by Dr. Paul Library on TodaysParent.com). sleep, then there is little incentive to learn to wake up and use
the toilet. There is also little incentive to learn to hold the urine for the
entire night. Diapers may thus prolong nighttime wetting. (See article
by Dr. Paul Library on TodaysParent.com).
Diaper "fetish", which may be either sexual or non-sexual, appears
to be common. Searching on the term "diaper lover" with  the Google search engine produces
60,000
results. Fetishes may start even at a young age. Emotional attraction
to diapers, which is called
"infantilism", also appears to be quite common. Searching on the term "infantilism" with the Google search engine produces
30,000
results. Many children, teenagers, and even adults, say that diapers "calm" them or induce a feeling of
"comfort" or "security". Emotional attraction to diapers may also be associated with fantasizing about being
treated as an infant and even desiring to use other infantile items such as pacifiers, baby bottles,
car seats, cribs,
etc. This may sound bizarre, but it is very real and appears to be quite
common. Healthcare providers seem unaware of this phenomenon.
There is nothing in the medical literature (Medline) about it. Until the Internet
came along diaper attraction and diaper fetish were apparently "closet" behaviors. The Internet has allowed these individuals with emotional
attachment to diapers and diaper fetish to come forth anonymously, without having to reveal their identities. Half of the postings on our bulletin boards
(which we filter out) indicate diaper attraction or diaper fetish.
Such postings typically ask, "Is there anyone else out there like me?". Furthermore, some kids say that the reason they stopped wetting was because, "I got tired of diapers." the Google search engine produces
60,000
results. Fetishes may start even at a young age. Emotional attraction
to diapers, which is called
"infantilism", also appears to be quite common. Searching on the term "infantilism" with the Google search engine produces
30,000
results. Many children, teenagers, and even adults, say that diapers "calm" them or induce a feeling of
"comfort" or "security". Emotional attraction to diapers may also be associated with fantasizing about being
treated as an infant and even desiring to use other infantile items such as pacifiers, baby bottles,
car seats, cribs,
etc. This may sound bizarre, but it is very real and appears to be quite
common. Healthcare providers seem unaware of this phenomenon.
There is nothing in the medical literature (Medline) about it. Until the Internet
came along diaper attraction and diaper fetish were apparently "closet" behaviors. The Internet has allowed these individuals with emotional
attachment to diapers and diaper fetish to come forth anonymously, without having to reveal their identities. Half of the postings on our bulletin boards
(which we filter out) indicate diaper attraction or diaper fetish.
Such postings typically ask, "Is there anyone else out there like me?". Furthermore, some kids say that the reason they stopped wetting was because, "I got tired of diapers."
Kids who are emotionally attracted to diapers or have diaper fetish many times
have one of two histories: 1) Their parents continued to change their
diapers when the child was older and even a teenager, or, 2) Their parents abused and
punished the child because of bedwetting. Having their diaper changed can
stimulate a child or teen sexually or can emotionally pull the child or teen back into the
security of being an infant. It is therefore a good idea to teach a child
to change his/her own diapers as soon as possible, even if occasional leaks
occur. Even 8 year olds can learn to change their own
diapers.
If a child is punished for wetting the bed and being put in diapers stops the
wet bed and the punishment,
the child may fear return of the punishment if diapers are removed. Emotional
attachment to diapers may then result. Also, a child who is abused
because of bedwetting may yearn for diapers because of the feeling of infantile
comfort and security
induced by a diaper.
 A child should take responsibility for
his/her bedwetting. It is a good idea to have the child change the sheets, and wash them, or at
least help with this. It appears that total acceptance of a child's
bedwetting by the parent does not induce incentive to become dry. Some
negative reaction by the parent seems productive. Physical or emotional
punishment, however, may not only be psychologically harmful to to the child,
but may actually prolong the wetting. Moreover, positive reinforcement for
dry nights also appears productive.. Implementation of a reward system, e.g. 2 chips for being
dry and taking away one chip for being wet may provide incentive to stop wetting
and get out of diapers. The chips can be exchanged
for video games, trips, etc. A child should take responsibility for
his/her bedwetting. It is a good idea to have the child change the sheets, and wash them, or at
least help with this. It appears that total acceptance of a child's
bedwetting by the parent does not induce incentive to become dry. Some
negative reaction by the parent seems productive. Physical or emotional
punishment, however, may not only be psychologically harmful to to the child,
but may actually prolong the wetting. Moreover, positive reinforcement for
dry nights also appears productive.. Implementation of a reward system, e.g. 2 chips for being
dry and taking away one chip for being wet may provide incentive to stop wetting
and get out of diapers. The chips can be exchanged
for video games, trips, etc.
Bedwetting probably does not cause diaper fetish or emotional attraction to
diapers. But being put back in diapers for bedwetting may trigger an
attachment or a fetish, if the child has the tendency. And once diaper
attachment or fetish is triggered, the child may continue to wet in order to
remain in diapers. Moreover, children with a subconscious desire to be in diapers,
who are dry for many years, may start to wet again on purpose, in order to pressure their parents into putting or keeping them in diapers.
How do you know if your child has emotional attraction to diapers or a diaper fetish? Ask these simple questions: 1)
Does your child seek or ask for diapers? Typically kids have to be pushed
into diapers. 2) Does he/she not want to try other ways of dealing with
bedwetting, such as medication or trying an alarm? 3) Does he
masturbate in his diapers? 4) Does he/she seek baby items such as toys or
pacifiers? In children who have emotional attachment to diapers or diaper fetish, social embarrassment at wearing diapers may eventually overcome the
attachment. Diaper attachment in teenagers creates a social
conflict. But in some individuals the attachment may be so strong that the behavior persists even into
adulthood. If you suspect that your child is wetting because of
diaper attachment or fetish, a child psychologist/psychiatrist may be able to
help.
 It can be argued that
attraction to diapers or diaper fetish is not harmful
to the child or teen, and should just be tolerated. But the behavior can be quite
distressing for the child's family and for healthcare professionals trying to treat
the wetting problem. The risks of testicular temperature elevation due to diapers are discussed above. Moreover, children who are wetting in order that they may wear diapers may be put through hazardous diagnostic procedures, such as cystograms, intravenous pylegrams's, x-rays, etc., and may be treated with potentially hazardous medications. Furthermore, the resulting social problems are
obvious. Teasing and impairment of relationships may result. Adults with diaper attachment/fetish even seek psychiatric help
because of the impact of the problem on relationships. It can be argued that
attraction to diapers or diaper fetish is not harmful
to the child or teen, and should just be tolerated. But the behavior can be quite
distressing for the child's family and for healthcare professionals trying to treat
the wetting problem. The risks of testicular temperature elevation due to diapers are discussed above. Moreover, children who are wetting in order that they may wear diapers may be put through hazardous diagnostic procedures, such as cystograms, intravenous pylegrams's, x-rays, etc., and may be treated with potentially hazardous medications. Furthermore, the resulting social problems are
obvious. Teasing and impairment of relationships may result. Adults with diaper attachment/fetish even seek psychiatric help
because of the impact of the problem on relationships.
Emotional attraction
to diapers or diaper fetish could
account for why many kids do not respond to treatments for both nighttime and daytime wetting (such as
alarms or medication), why kids start wetting again when they have been dry for several
years, and why kids wet more when they are under emotional stress. The
Internet appears to be revealing the tip of an iceberg. Healthcare providers who evaluate
children and teenagers for wetting should therefore rule out emotional attraction
to diapers or diaper fetish as the cause, before potentially harmful procedures and treatments are carried out.
Moreover, underlying psychological problems should be looked for. Organized
scientific investigation is needed to fully understand the role that emotional attraction
to diapers and diaper fetish play in nighttime wetting and daytime wetting.
|
Things To Do To Help The Child Who Bedwets |
1. Make sure that your child uses the toilet before going to bed.
2. Don't give your child fluids for a few hours before bedtime. Especially avoid caffeine drinks like tea and colas during that same time.
3. Children can not willfully control bedwetting, although they can usually
learn to stop. Don't scold your child excessively, but encourage him/her to work
on a treatment plan. Don't punish your child for bedwetting and do not call him/her
names: ("Only babies wet their beds.")
4. For an older child have him/her change his/her clothes and bed linen.
It is important for
the child to assume
some responsibility, so that they focus on the problem.
5. Continuation
of diapers may not be a good idea for "curing" your child of bedwetting, especially during the time when a child is using an alarm. If the child is using diapers he/she may not be motivated to stop urinating at the alarm or get up and go to the toilet.
Instead use plastic sheets with
a cotton sheet over the plastic covering. Two layers of plastic and sheets
can allow you to remove one layer if the child wets in the night without having
to re-make the entire bed.
6. Be supportive and reassure your child that he/she will be able to gain control of his/her bladder.
7. Bedwetting is thought by many health professionals to occur during very deep
sleep. Stress appears to make wetting worse, perhaps because the child is more
tired and sleeps
more deeply. Avoid letting your child become overly tired. Decreasing extracurricular activities may be
necessary, especially during the treatment period.
8. Water beds are a way to have a wet-resistant mattress that is much more
tolerable to the child than a plastic cover. Water beds are cooler, do not
crackle (your child's friends won't know about the bedwetting), and they are easy to clean.
9. Stopping bedwetting is like getting into shape. It requires that both the child and parents buy into the idea and commit to
a treatment.
10. If your child has a problem holding his or her urine during the day or has been completely dry at night for several months and then begins wetting
the bed, there may be other physical problems, such as diabetes or a urinary tract infection.
See your family doctor and have your child checked. And if bedwetting is really upsetting either you or your
child, no matter what the age, it is a good idea to talk to your doctor about it.
| Children's Hospital Night
Time Wetting Strategies* |
1) Limit fluids two hours before bedtime if possible.
If the child is involved in sports in the evening, they should be allowed to drink
water to replace fluids lost during activity.
2) The child may have 2 oz of water when they brush their
teeth. A
good
couple of swallows is okay, but avoid drinking a large glass right
before bed.
3) Make sure the child
goes to the bathroom twice before bed. They
will then start out with "an empty tank." Have them go potty
30 minutes before bed and go again right before bed. Because we only feel our
bladder when its full, they will need to have an adult remind and/or monitor
them as they will not feel like they need to go. Make this a part of the bedtime
routine.
4) Make sure the child
is not constipated. They should go to the bathroom for a bowel movement daily or
at least every other day. If they are constipated, their bladder will likely have a
decreased capacity and not be able to hold as much as it should. If you think
your child is constipated have them drink more water and eat more raw fruits and
vegetables to increase fiber. Popcorn and raisin bran are easy ways to increase
fiber in a child's diet. If this does not help, talk with your health care
provider for further assistance.
5) Try giving your child a sport bottle of water to take to
school (24-32 oz). Have them drink all of it by about 1:00 in the
afternoon (you may flavor the water with vanilla, lemon, or 1 oz apple juice or
white grape juice). This will help make sure the child does not "load
up" on fluids late in the
day, i.e., after school because they have come home dehydrated from their day's
activities
6) Have the child say out loud at bedtime,
"l'm going to wake up tonight to go to the bathroom! " and ask them to
picture themselves doing this. Make sure there
is a clear path to the bathroom so the child will be able to get there easily,
i.e.,
night lights, etc.
*Cathy Cornell, A.R.N.P., Enuresis Clinic, Dept. of Urology, Children's Hospital and Medical
Center, Seattle, WA.
© 1999,
2000, 2001, 2002, 2003 Children's Hospital and Medical Center, Seattle,
WA.
References:
1. Rappaport, L., Evaluation of
the wet child., American Academy of Pediatrics National Meeting and Exposition,
San Francisco, October 2001.
2. NEVÉUS, T.,
Oxybutynin, desmopressin and enuresis., THE JOURNAL OF UROLOGY
2001;166:2459-2462
3. Hinde,
M., Hjertonsson, M., and Broberg, A.: Low self-esteem of children with enuresis.
Mental and social health compared in different groups. Psykologiska.
Institutionen., Goteborgs universitet. Lakartidningen, 92: 3225, 1995.
Disclaimer:
The information contained
above should not be used as a substitute
for the medical care and advice of your physician.
There may be variations in treatment that your
physician may recommend based on individual facts
and circumstances. Please read full disclaimer.
© 1999,
2000, 2001, 2002, 2003 eHealth
International, Inc.
|
 Bedwetting, which is also called enuresis (pronounced
"en-yur-ree-sis"), affects over 7 million children in the United
States. This is about one out of seven children between the ages of 5 and 18.
The rate in other
countries appears to
be similar, which calculates to almost 200 million kids wordwide. Fortunately, each year, as a child grows, Mother Nature cures about 15% of
the kids affected. Thus, most children with bedwetting will "out-grow" it. But
during the time when a child has the problem it can seriously affect his or
her life as well as that of the family. And 3% do not outgrow it!
Bedwetting, which is also called enuresis (pronounced
"en-yur-ree-sis"), affects over 7 million children in the United
States. This is about one out of seven children between the ages of 5 and 18.
The rate in other
countries appears to
be similar, which calculates to almost 200 million kids wordwide. Fortunately, each year, as a child grows, Mother Nature cures about 15% of
the kids affected. Thus, most children with bedwetting will "out-grow" it. But
during the time when a child has the problem it can seriously affect his or
her life as well as that of the family. And 3% do not outgrow it!